
Any time guns are involved by one or more parties, there’s a reasonable chance a concealed carrier is apt to take a bullet. Most states require some form of firearms training prior to getting that concealed carry permit but none that we know of require any training in emergency first aid. As we discussed in a previous article, one of the biggest threats of receiving a gunshot wound is blood loss. The human body only needs to lose, on average, about a third of his total volume of blood before unconsciousness and death set in. There are plenty of exceptions but that’s a good guideline.
After being shot, it’s important to take a few things into account:
Pre-Amble To Receiving First Aid
In Detroit, Michigan, it takes the police – on average – 24 minutes to respond to a call. In New York City, that number drops to 8 minutes. In an urban environment, if you are shot in the leg, you can usually expect first responders to arrive within the half hour. In less densely populated areas or rural environments, that time can increase to as much as 40 or more minutes.
According to the Bureau of Labor Statistics, there is roughly 1 full-time police officer for every 650 people in the United States. So, that’s a pretty light density. Most full-time police officers are trained in some form of emergency first aid. If shot, most will attempt to assist you after they’ve secured the scene…
…After they’ve secured the scene.
When police arrive, they don’t know immediately if you’re a good guy or a bad guy. If you’re a concealed carrier who’s just been shot, you’re probably armed. It will take that police officer seconds or minutes to determine he’s safe to approach you to perform first aid on your gunshot wound… If he doesn’t decide that it would be safer for him to stand by and wait for paramedics to arrive.
Conclusion? If you’re shot in the leg and waiting on emergency services, you need to be prepared to sit tight.
Gunshot Wounds To The Leg
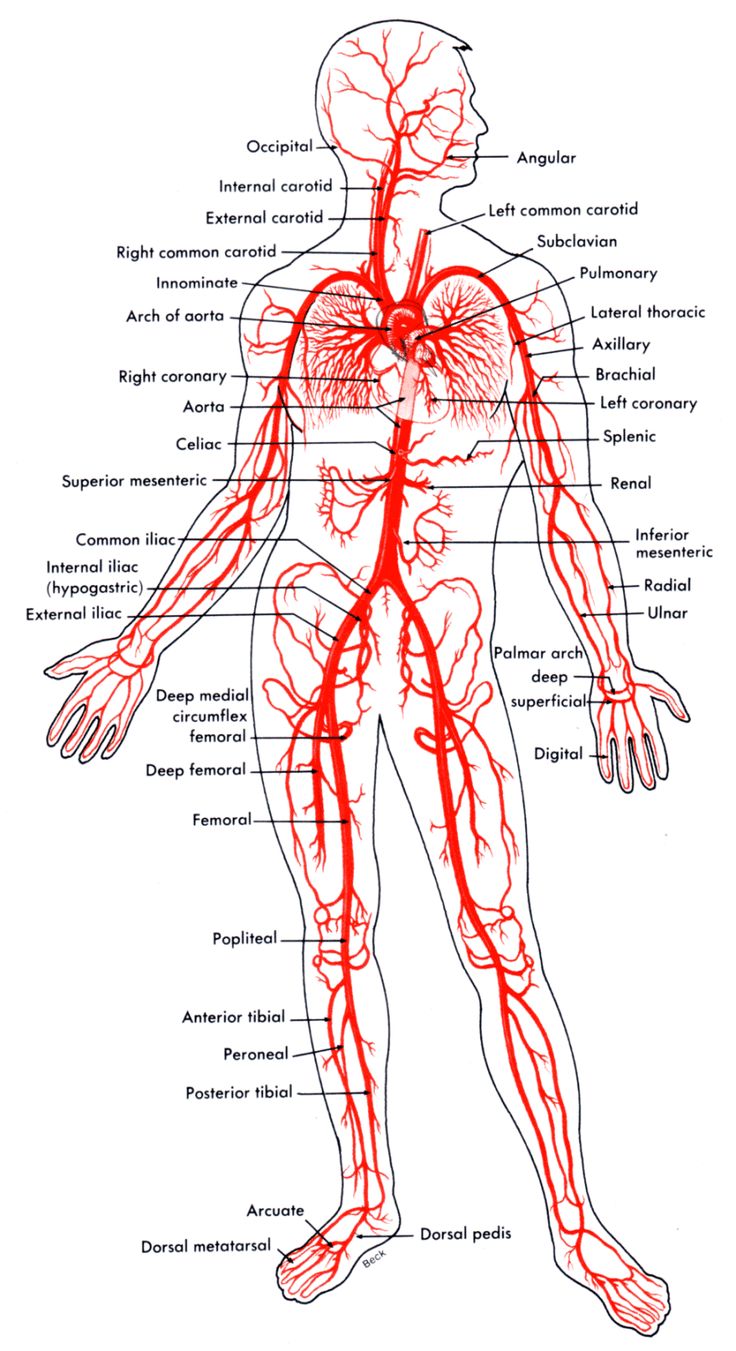
Now, let’s talk about that leg. We’re enclosing a basic layout of the circulatory system of the human body – but let’s focus on the area in and around the leg.
Danger Zone: Upper To Mid-Thigh
The two worst places to get hit are in the center and inner thigh. Shielded by layers of muscle, fat, and bone, there is an extremely powerful system of arteries coursing through the upper and lower thigh – the femoral arterial system. Good news? It’s possible to take a bullet through the fatty portion of your inner thigh and luck out. Bad news? If the femoral artery is nicked or severed – you won’t likely be conscious long enough to worry about the rest.
The outer thigh is fair game – assuming the bullet enters and exits through the outer thigh. There are arterial systems that stretch into this region but they are no where near as major and catastrophic as the main femoral arterial system. It still has the possibility of being lethal and should be taken extremely seriously.
If you take a direct hit or even knick one of these arteries in the femoral system, you will bleed out very quickly (minutes – not hours). How do you know if your femoral artery has been hit? Your body will be ejecting a lot of blood at a very fast rate.
- Your absolute priority is to stop the bleeding. Depending on the wound channel, this may be as simple as plugging it with a finger or thumb to slow the rate while you or another apply emergency first aid. If you are able – elevate that leg above your heart as fast as possible.
- Laying on your back, prop your leg against a wheel, a chair, the side of a car or building – ANYTHING that keeps it pointing above the plane of your heart. You want to slow down the rate of flow to that leg.
- Apply strenuous direct pressure to the wound.
You don’t always need a tourniquet! You determine the need for a tourniquet by medical training and observation.
Case In Point: This woman was shot in the thigh and didn’t even realize she had been shot. The bullet was lodged near her femoral artery but did not sever it. Bleeding, as you can see from the article – was minimal. This is not in any way normal – but it is an example where you may not need a tourniquet to treat for gunshot wounds to the thigh.
If you are going to apply a tourniquet, you’re going to need to place it at the closest available joint above the wound. In the case of an upper thigh gunshot wound where you strongly suspect the femoral artery has been severed or severely damaged… Let’s be honest, someone else is applying the tourniquet.
People who have been trained in battlefield first aid and emergency first aid through either the military, law enforcement, or emergency medical training understand at least the very basics to spotting a suspected wound to the femoral artery.
Also, big caveat: just because someone sees you’ve taken a gunshot wound to the upper thigh and blood is gushing out like mad doesn’t mean they’ll do a single thing to stop it. Even though any bystander is mostly covered by the Good Samaritan clause, that doesn’t mean they want to take responsibility for your injuries. It also doesn’t mean they have any clue what they’re doing. IF you have training, you can at least be in the position to talk them through it.
Incorrectly applying a tourniquet is arguably as bad as leaving the wound alone.
The rate of blood loss from the extremities can generally be staunched (usually not completely stopped) by the application of a tourniquet. A tourniquet is not the only way to slow blood loss.
Once that tourniquet goes on, the clock starts ticking down to when you lose that limb. That time can be anywhere from over an hour to upwards of four hours depending on a number of factors including:
- The skill of the person applying it
- The material used for the tourniquet
- Your own personal physiology
Peer-reviewed medical journal findings on the matter of how long a tourniquet can be applied without losing a limb:
Preventing arterial blood flow to a limb will result in ischaemia. Continuous application for longer than 2 h can result in permanent nerve injury, muscle injury (including contractures, rhabdomyolysis and compartment syndrome), vascular injury and skin necrosis.8 Muscle damage is nearly complete by 6 hours, with likely required amputation. Numerous studies have been performed to determine the maximum duration of tourniquet use before complications. The general conclusion is that a tourniquet can be left in place for 2 h with little risk of permanent ischaemic injury. However, the majority of the literature looks at pneumatic tourniquets in elective theatre cases with normovolaemic patients. In hypovolaemic trauma patients with non‐pneumatic tourniquets these figures may not be applicable. There is very little data on the complication rate of clinically indicated pre‐hospital tourniquet application and therefore there is no safe tourniquet time. Lakstein identified that 5.5% of 110 pre‐hospital tourniquet applications resulted in neurological complications, with an ischaemic time between 109–187 min. None of these resulted in limb loss. The mean ischaemic time for use of a tourniquet with no complications was 78 minutes.
Tourniquet use in the civilian prehospital setting, Lee, C, Porter, K M, Hodgetts, T J, Emerg Med J. 2007 Aug; 24(8): 584–587,
Not to be a debbie-downer, but that’s going to be the least of your concerns.
For an upper thigh wound, if you need to apply that tourniquet, apply it above the wound at the nearest joint. So, your hip socket. It does little good to apply a tourniquet to the meaty portions of your thigh because you have a lot of fat and tissue that the other person will have to compress to squeeze off the artery.
Let’s be perfectly clear: take some EMT basic classes at your local community college if you want to actually be able to help in this sort of situation.
We’ve included this video of a former Corpsman (Navy medic), USMCDoc14. He’s a bit callous and sometimes uses foul language and this video is JUST for educational purposes only. Attend formal training if you actually have any expectation of successfully applying a tourniquet. Also, check out his videos on how to fabricate an AK-47 from near scratch – off-topic but still great for educational purposes.
Past The Knee: More Options
The femoral artery can still be nicked or severed with a gunshot wound in the vicinity of the knee. And if so, you will bleed out very quickly.
- You’re going to want to elevate the leg above your heart. Prop it up so it’s above the plane of your heart.
In the case of a gunshot wound, it’s important to determine entrance and exit. If it entered and left in roughly the same area – great! However, that’s not always the case. Sometimes bullets exit in a completely different area. Sometimes the bullet is lodged inside.
If you’re on your own, you may not be able to determine this by yourself. However, this information is extremely important because it does you no good to stop the blood loss from one wound while a second (or third or fourth) one is pouring out equally fast.
Once you’ve determined entrance and exit
- and your leg is elevated above the heart,
- you or someone else is applying direct pressure to both the entrance and exit wounds,
…you may then determine you need to apply a tourniquet. Blood loss and prior medical training will help you determine if that’s necessary. It’s possible to get shot in the lower leg (or any extremity) and not need a tourniquet. This is why medical training is good.
If the knee was shot — if you need to apply the tourniquet, apply it above the knee and at the joint where the knee and lower thigh meet.
If the shot was below the knee — apply it at the nearest joint above the entrance and exit wound. So, if you were shot in the shin but the bullet somehow exited through the back of your knee – you’re back to applying the tourniquet to the joint where the thigh and knee meet.
If the tourniquet is not above the wound channel (i.e. between your wound and the pathway to your heart), it’s not going to help.
Sometimes, simply applying direct pressure may be sufficient to staunch an open wound channel until medical assistance arrives.
If you do apply a tourniquet, you’re going to want to tie off the torque bar on the tourniquet so it can’t move. If you’re still conscious, you probably did something right. Write the time you applied the tourniquet on a conspicuous place. In the Marines, we put this right on the forehead and/or applied tape to the uniform with the time and blood type. If you know your blood type, write that, too. If you lose consciousness between now and when medical services arrive, both pieces of information will be very handy.
This article is mostly to give you an idea of the sort of emergency medical care you will be expected to apply to yourself (or another) in the event of a self-defense scenario where one or more of you are shot in the leg. This is not medical training. There is no substitute for medical training. And you should always seek professional medical help for any injury you receive.
The bigger question remaining: do you have a first aid kit on hand that can be used to treat these sorts of injuries? If the answer is no, it’s definitely something to consider. Some components that should always be included:
- a tourniquet with a torque bar
- sterile gauze
- wraps
- a black, permanent marker
- antibiotic ointment
- isopropyl alcohol (1 L)
- cotton swabs
- field dressing
- sterile surgical stapler with staples
- neck brace
- leg brace
Always a good idea is to include a piece of paper to keep track of the inventory. This doesn’t need to be your carry first aid pack but it’s definitely something to consider keeping in your vehicle.
When medical services arrive, try to give them as much pertinent information as you’ve determined – entrance and exit of the bullet, time of application of tourniquet, blood type, name – anything that can be used to treat your injuries faster.